Physical Therapy Guide to Congenital Heart Defects
Congenital heart defects are the most common type of birth defect. They occur in about 1% of births each year. CHDs affect the normal structure of the heart and the way it works.
Young children and teens with CHD often need physical therapy due to problems meeting motor (movement) milestones, decreased tolerance for play and activity, or to address the effects of surgery.
Physical therapists are movement experts who use the latest evidence to design treatment plans for each person’s needs and goals. They improve quality of life through hands-on care, patient education, and prescribed movement. You can contact a physical therapist directly for an evaluation. To find a physical therapist in your area, visit Find a PT.
What Is a Congenital Heart Defect?
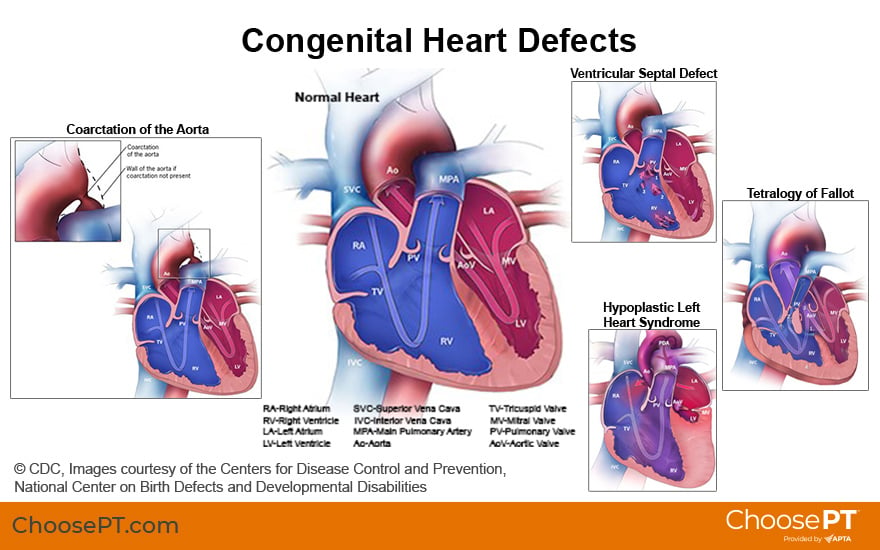
To understand CHDs, it may help to first review normal blood flow through the heart. The heart has four hollow chambers. They are the:
- Right atrium.
- Right ventricle.
- Left atrium.
- Left ventricle.
Heart function and disease are generally referred to in relation to the right and left sides of the heart.
In a healthy heart, blood travels through the right atrium and right ventricle then into the lungs. In the lungs, blood picks up oxygen and becomes oxygenated. It then travels back to and enters the left side of the heart. The oxygen-rich blood travels through the left atrium and left ventricle. It then gets pumped to the rest of the body through a large blood vessel (tube) called the aorta. After delivering oxygen throughout the body, the blood, which is now depleted of oxygen, returns to the right side of the heart to repeat this continuous process.
With CHD, this normal blood flow is altered or the work of the heart becomes more difficult. The path may be altered inside the chambers of the heart or at the vessels (tubes) carrying the blood to and from the heart.
There are two categories of CHD:
Acyanotic
Acyanotic heart defects typically do not impact oxygen levels delivered throughout a child’s system/body.
With an acyanotic defect, blood travels normally from the right side of the heart to the lungs. However, when it returns to the left side of the heart, some blood goes to the rest of the body as normal, and some also travels back into the right side of the heart without going to the body first. This is also known as “left to right shunting.” With an acyanotic defect, the child does not generally have a bluish (cyanotic) tint to the skin. But a bluish tint may appear on the skin during activities that require more oxygen (such as crying and feeding).
Examples of acyanotic defects include:
- Ventricular septal defect, or VSD, is the most common CHD; it occurs in 1 out of every 240 births in the United States. A VSD is a hole between the two lower chambers (ventricles) of the heart. Small VSDs may close on their own. Medium or larger holes can lead to left to right shunting, the need for surgery, and possible heart failure.
- Patent ductus arteriosus, or PDA, occurs in 1 out of every 2,000 births in the U.S. Before birth, all babies’ hearts have an opening called the ductus arteriosus. This opening, between the aorta and the pulmonary artery, allows oxygen-rich blood to flow to the body while diverting blood from the baby’s lungs while in the womb. When a baby is born and begins breathing on its own, the ductus arteriosus closes, and blood flows to the lungs to pick up oxygen. Typically, the ductus arteriosus closes within a few days after birth. When it does not, it is called a patent (meaning “open”) ductus arteriosus. With a PDA, some oxygen-rich blood travels from the heart to the body, but some also flows back into the lungs instead. A PDA can be caused when a newborn has low blood oxygen levels. This is one reason why CHD occurs more often in babies who are born too soon (premature).
- Narrowing (coarctation) of the aorta. Coarctation of the aorta occurs in 1 out of every 1,800 births in the U.S. This narrowing of the aorta can block or slow blood flow. This makes it harder for the heart to pump blood out of the left side of the heart into the body. It can cause higher blood pressure in the arms and lower blood pressure in the legs. The extra work and higher pressures can lead to an enlarged left side of the heart. Surgery to widen or bypass the narrow area may be needed.
Cyanotic
Cyanotic heart defects cause a mixing of oxygen-rich and oxygen-deprived blood in the body. With cyanotic defects, the blood enters the right side of the heart, but leaves the heart before going to the lungs for oxygen. This is a problem because all parts of the body — from the brain to the muscles — need oxygen to function. The lack of enough oxygen-rich blood causes a bluish (cyanotic) color of the skin, lips, and nails.
Examples of cyanotic defects include:
- Hypoplastic left heart syndrome, or HLHS, the left ventricle is most noticeably smaller or less developed than typical. HLHS occurs in 1 out of every 3,841 births in the U.S. Other heart structures tend to be less developed as well. This leaves only the right side of the heart (right ventricle) fully functional. If the infant also has other heart defects, such as a VSD or PDA, these defects are left open on purpose to allow better blood flow until surgery to repair HLHS can occur. Surgery for HLHS has three stages; the first occurs when the baby is only a few days old.
- Tetralogy of Fallot, or TOF, is the most common complex defect and occurs in 1 out of every 2,518 births in the U.S. It consists of four problems:
- A VSD.
- A narrowing of the pulmonary valve (the path blood takes to get to the lungs and the muscular area beneath it).
- A thickening of the right ventricle.
- An abnormal position of the aorta that can decrease blood flow to the lungs.
While CHD may occur without any related health conditions, they often occur alongside other conditions or syndromes, including:
- Premature birth.
- Down syndrome.
- DiGeorge syndrome.
- Williams syndrome.
- Fetal alcohol syndrome.
- Other genetic disorders.
Additional complications of CHD may include:
- Heart failure or infections.
- Stroke.
- Heart rhythm problems.
- Limited ability to take part in or enjoy physical activity.
- Increased risk of obesity.
- Behavioral changes.
- Developmental delays.
Signs and Symptoms
Children with CHD have a variety of symptoms linked to the size and type of defect. For example, a newborn with a small VSD may not be diagnosed or show symptoms until childhood. However, a newborn with a large defect may have trouble feeding, and therefore:
- Receive an early diagnosis.
- Undergo surgery within the first months of life.
Common symptoms of CHD in a newborn include:
- Fast heart rate.
- Increased irritability.
- Trouble breathing.
- Sweating or getting tired with feeding.
- Trouble gaining weight.
- Swelling around eyes, belly, or legs.
Common symptoms in childhood include:
- Passing out during play.
- Feeling their heart race.
- Feeling chest pain.
- Having trouble breathing when playing.
- Swelling of the hands, ankles, or feet.
How Is It Diagnosed?
Medical doctors may diagnose CHD during pregnancy, early after birth, in childhood, or even in the teenage years. If possible, diagnosis during pregnancy allows for proper planning of any needed surgery and early medical management. This is especially important for children with cyanotic defects.
Smaller defects may not get diagnosed or may not need repair at birth. You should talk to your pediatrician or cardiologist if your child shows any of the following symptoms:
- Having trouble breathing.
- Feeling as though their heart is racing.
- Having chest pain when playing with peers or during sports or other physical activity.
How Can a Physical Therapist Help?
After medical diagnosis of a CHD, a physical therapist can partner with other health care providers to help you and your child better understand their condition. Physical therapists promote development and help children progress with physical function.
A physical therapist will perform an evaluation that includes:
- A thorough review of the medical history including heart structure, medications, surgeries, as well as any available test results and imaging.
- Discussion of family routines, concerns, and goals.
- Developmental assessment based on the child’s age.
- Muscle strength and flexibility testing.
- Walking or running tests to measure exercise capacity.
- Tests of coordination and balance.
- Monitoring of breathing and heart rate.
With input from the you and your child, and while partnering with the medical team, the physical therapist will design a treatment plan specific to your child’s needs and goals. Your physical therapy plan may include:
Education. Your physical therapist will design and teach you how to do a home exercise program. They also will recommend lifestyle changes and teach you and your child how to manage their condition. Physical therapists also may explain any concerning signs and symptoms to watch out for during rest and activity.
Playtime. Babies with CHD are at risk for developmental delays. Your physical therapist can work with you and your child to ensure proper activities to support tummy time, rolling, and reaching. They will show you how to engage your newborn in play activities that help with rib cage development as they grow. This is particularly important if your child had heart surgery that required opening their chest. Physical therapists also can help children reach their walking milestone more quickly and work with them to improve activity tolerance.
Aerobic exercise. People with CHD are at risk for low exercise tolerance in childhood and adulthood. A physical therapist can design and monitor a personalized exercise program to help increase aerobic endurance. An aerobic exercise program improves physical activity tolerance and quality of life. Physical therapists help children and families explore various forms of aerobic exercise, such as walking, dancing, biking, or using obstacle courses. Finding an enjoyable physical activity is important for anyone, especially people with CHDs.
If Surgery Is Needed
Many CHDs require surgery to repair them. A physical therapist may see the child before, after, or between surgeries:
Before surgery. A physical therapist may complete a baseline assessment of development or fitness. They will provide education on movement after surgery.
After surgery. A physical therapist can:
- Educate caregivers on how to safely handle and position a newborn after surgery.
- Advise on safe playtime, walking, and movement after surgery.
- Promote improved breathing patterns and upper body movement.
- Support a return to presurgery functioning.
- Assist with scar healing.
Between surgeries. Some CHDs, such as HLHS, involve a series of staged surgeries. A physical therapist will help with the motor development and functional endurance needed to both recover from, and prepare for the next, surgery.
Some hospitals offer outpatient pediatric cardiac rehabilitation. Cardiac rehab is a program for people who are recovering from heart disease, heart failure, and heart surgery. Medical professionals, including physical therapists, run this structured program of physical conditioning and lifestyle counseling. Participating in an outpatient pediatric cardiac rehab program has been shown to:
- Increase physical activity, which is important for overall health, especially for people with heart conditions.
- Improve development and cognition.
- Promote healthy lifestyle habits.
- Improve quality of life.
Can This Injury or Condition Be Prevented?
The exact cause of CHDs is unknown. There are some reported environmental and genetic factors that may increase the risk of CHD:
- Rubella infection during pregnancy.
- Uncontrolled maternal diabetes.
- Smoking or alcohol intake during pregnancy.
- Family history and genetics.
- Medications taken during pregnancy.
Because people with CHD may avoid physical activity and resort to frequent sitting, they are at an increased risk for other health issues, such as obesity. Physical therapists provide important support to establish healthy habits from an early age.
What Kind of Physical Therapist Do I Need?
All physical therapists are trained through education and experience to evaluate, manage, and treat various symptoms and conditions. Families with children who have CHD may want to consider:
- A physical therapist experienced in treating individuals with CHD.
- A physical therapist who is a board-certified clinical specialist in pediatrics, cardiovascular and pulmonary physical therapy, or a physical therapist who has completed a residency or fellowship in pediatrics or cardiovascular and pulmonary physical therapy. These physical therapists may include PCS or CCS after their name on business cards or on their website profile. Physical therapists with these qualifications have advanced knowledge, experience, and skills to treat children with CHD.
- A physical therapist who has a practice that focuses on pediatrics or cardiovascular and pulmonary physical therapy, including a formal pediatric cardiac rehabilitation program (usually associated with a hospital).
You can find physical therapists in your area with these credentials and clinical expertise on Find a PT, a tool built by the American Physical Therapy Association.
General tips when you're looking for a physical therapist (or other health care provider):
- Ask family, friends, or other health care providers to recommend a physical therapist.
- Ask about the physical therapist’s experience treating children with congenital heart defects before you make an appointment.
- Be prepared to describe your symptoms in as much detail as possible, including what makes symptoms worse or better.
The APTA Academy of Pediatric Physical Therapy contributed to this consumer resource. It is for information purposes only and is not intended to represent the position of APTA Pediatrics.
The American Physical Therapy Association believes consumers should have access to information to:
- Inform their health care decisions.
- Prepare them for their visit with a health care provider.
The following resources offer some of the best scientific evidence related to physical therapy treatment for CHD. They report recent research and provide information on the standards of practice in the United States and worldwide. They link to a PubMed* abstract (which may offer free access to the full text) or to other helpful resources. You can read them to learn more or bring a copy to your health care provider.
American Heart Association. https://www.heart.org/en/health-topics/congenital-heart-defects. Accessed February 4, 2022.
Center for Disease Control and Prevention. Congenital heart defects. https://www.cdc.gov/ncbddd/heartdefects/index.html. Accessed February 4, 2022.
McBride MG, Burstein DS, Edelson JB, Paridon SM. Cardiopulmonary rehabilitation in pediatric patients with congenital and acquired heart disease. J Cardiopulm Rehabil Prev. 2020;40(6):370–377. Article Summary on PubMed.
Gauthier N, Curran T, O’Neill JA, Alexander ME, Rhodes J. Establishing a comprehensive pediatric cardiac fitness and rehabilitation program for congenital heart disease. Pediatr Cardiol. 2020;41(8):1569–1579. Article Summary on PubMed.
Akamagwuna U, Badaly D. Pediatric cardiac rehabilitation: a review. Curr Phys Med Rehabil Rep. 2019;7(2):67-80. doi:10.1007/s40141-019-00216-9.
Dagenais L, Materassi M, Desnous B, et al. Superior performance in prone in infants with congenital heart disease predicts an earlier onset of walking. J Child Neurol. 2018;33(14):894–900. Article Summary on PubMed.
Howell B, Tapley CD. Congenital heart conditions. In: Palisano RJ, Orlin MN, Schreiber J, eds. Campbell’s Physical Therapy for Children. 5th ed. St Louis, MO: Elsevier Inc; 2017:646–647, 659.
Longmuir PE, Brothers JA, de Ferranti SD, et al. Promotion of physical activity for children and adults with congenital heart disease: a scientific statement from the American Heart Association. Circulation. 2013;127(21):2147–2159. Article Summary on PubMed.
Mumtaz MA, Qureshi A, Mavroudis C, Backer CL. Patent ductus arteriosus. Pediatric Cardiovascular Medicine. 4th ed. Hoboken, NJ: Blackwell Publishing; 2013: 225–233.
Backer CL, Kaushal S, Mavroudis C. Coarctation of the aorta. Pediatric Cardiovascular Medicine. 4th ed. Hoboken, NJ: Blackwell Publishing; 2013: 256–282.
Tikkanen AU, Oyaga AR, Riaño OA, Álvaro EM, Rhodes J. Paediatric cardiac rehabilitation in congenital heart disease: a systematic review. Cardiol Young. 2012;22(3):241–250. Article Summary on PubMed.
Parker SE, Mai CT, Canfield MA, et al. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88(12):1008–1016. Article Summary on PubMed.
Hirth A, Reybrouck T, Bjarnason-Wehrens B, Lawrenz W, Hoffmann A. Recommendations for participation in competitive and leisure sports in patients with congenital heart disease: a consensus document. Eur J Cardiovasc Prev Rehabil. 2006;13(3):293–299. Article Summary on PubMed.
Hoffman JL, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890–1900. Article Summary on PubMed.
*PubMed is a free online resource developed by the National Center for Biotechnology Information. PubMed contains millions of citations to biomedical literature, including citations in the National Library of Medicine's MEDLINE database.
Expert Review:
May 17, 2022
Revised:
Jun 22, 2022
Content Type: Guide
Congenital Heart Defects
PT, DPT, board-certified clinical specialist in pediatric physical therapy, on behalf of the APTA Academy of Pediatric Physical Therapy
Ashley Parish
PT, DPT, board-certified clinical specialist in cardiovascular and pulmonary physical therapy and certified respiratory therapist