Physical Therapy Guide to Cubital Tunnel Syndrome
Cubital tunnel syndrome, or CuTS, is the second most common nerve problem in the arm. The most common is carpal tunnel syndrome. CuTS happens when there is too much pressure on a nerve in your elbow called the ulnar nerve.
This pressure can cause pain or discomfort in your elbow, forearm, and hand. It also can make your hand feel weak or clumsy. Symptoms often show up while you sleep (if your elbow is bent), when your elbow stays bent for a long time, or when you lean on your elbow.
CuTS is more common in people whose work or hobbies involve repeated or prolonged elbow movements, such as using hand tools, typing, painting, or playing instruments. The risk also may be higher in individuals who smoke, are male, or have underlying conditions like diabetes or cardiovascular disease.
Physical therapists can help people with CuTS feel better. They teach ways to avoid activities that make symptoms worse, reduce pain and swelling, and help you regain movement and strength.
Physical therapists are movement experts. They improve quality of life through hands-on care, patient education, and prescribed movement. You can contact a physical therapist directly for an evaluation. To find a physical therapist in your area, visit Find a PT.
What Is Cubital Tunnel Syndrome?
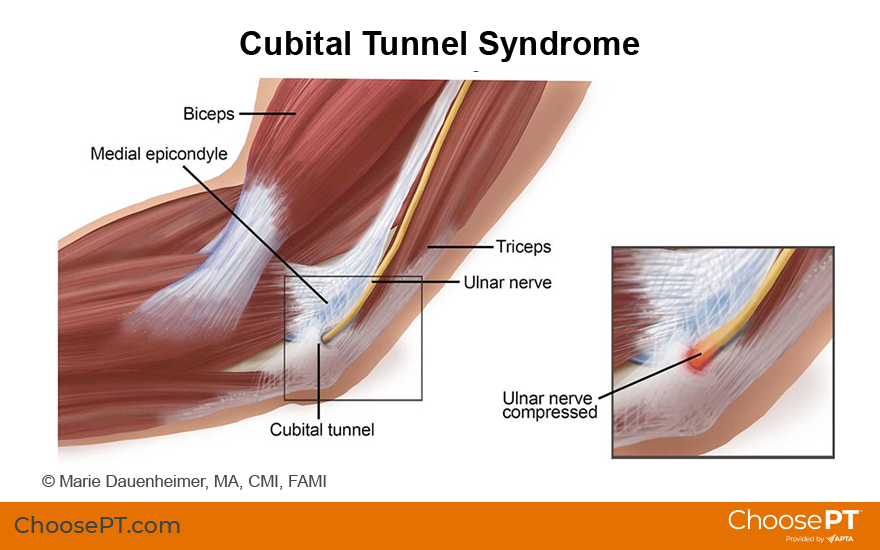
The cubital tunnel is a small space made of bone, muscle, and soft tissue that the ulnar nerve passes through near your elbow.
Cubital tunnel syndrome occurs when the ulnar nerve gets squeezed or stretched where it passes under the medial epicondyle, the bony bump on the inside of your elbow. If you have ever hit your “funny bone,” you have hit the ulnar nerve as it passes through the cubital tunnel. When you bump it just right, you might feel pain, tingling, or numbness running down your arm and into your hand. That feeling usually goes away quickly.
With CuTS, however, the pressure on the nerve happens more often and lasts longer. The symptoms may not feel as sharp as hitting your funny bone, but they tend to last longer and can worsen with certain daily activities.
CuTS also can happen when the nerve is stretched too much, like when your elbow is bent for a long time or moved repeatedly during the day. When your arm stays bent, the ulnar nerve gets pulled across the inside of your elbow, which can reduce blood flow and cause swelling and irritation in the nerve.
Signs and Symptoms
Initial symptoms of cubital tunnel syndrome may include:
- Pain and tenderness at the inside of the elbow
- Pain during sleep (if your elbow stays bent)
- Pain, numbness, and tingling that comes and goes in the inner forearm and hand, as well as the ring and pinky finger
These symptoms typically respond well to treatment but can advance to:
- Difficulty gripping and clumsiness
- Loss of muscle size and strength (atrophy) in the small muscles of the hand
- A hand condition in which the ring and pinky fingers bend toward the palm. This is called an "ulnar claw hand."
Caution: Severe symptoms, especially with muscle atrophy and hand deformities, should be evaluated by a physician.
How Is It Diagnosed?
Physicians or physical therapists can diagnose cubital tunnel syndrome. Your physical therapist will ask about your symptoms and how long you've had them. They will also observe how you move and assess your:
- Joint range of motion
- Strength and flexibility
- How well you can feel different types of pressure
Your physical therapist will conduct special tests to determine what is causing stress and pain in your elbow. They will use these findings to design the best treatment plan for you.
If a diagnosis cannot be made with these tests, your physical therapist will send you to your physician, who may refer you to have:
- Electromyography, or EMG, to assess the health of a muscle, and a NCS, or nerve conduction study, to assess the function of a nerve. These tests are typically performed by physical therapists with a clinical electrophysiology specialty or neurologists with training in neuromuscular medicine or electrodiagnostic medicine.
- Ultrasound: looks to see where your nerve may be getting squeezed
- MRI: helps rule out other causes of your symptoms
How Can a Physical Therapist Help?

If you have a mild or moderate case of cubital tunnel syndrome, physical therapy can help improve your symptoms.
At first, the goal of physical therapy is to reduce how often and how badly your symptoms happen. This part of treatment may include:
- Changing some of your daily activities to take pressure off your arm
- Wearing a brace or using tape to help your arm heal
- Using heat, ice, or other treatments to reduce pain and swelling
- Learning better ways to move, sit, or work to protect your arm
- Having hands-on therapy to relax tight muscles and help you move more easily
- Doing gentle stretches and exercises to improve flexibility and nerve movement
- Performing light resistance exercises to help your muscles heal and get stronger
As you start to feel better, your physical therapist will slowly add more challenging exercises. This helps make sure your symptoms don’t come back when you return to normal activities. This part of therapy may include:
- Exercises to fix muscle imbalances and improve how you move
- Slowly adding more stress to your arm to build strength and endurance
- Carefully returning to your regular activities while watching how your body responds
During your recovery, your physical therapist will keep checking how you’re doing, how well you move, and how your symptoms are changing. The goal is to help you meet all your treatment goals and get back to your normal activities without pain.
If Surgery Is Required
Sometimes, surgery is needed for more serious cases of cubital tunnel syndrome. This may happen if other treatments like changing activities, wearing braces, doing physical therapy, or taking medicine haven’t worked after six months. Surgery also may be needed if the muscles in your hand have gotten smaller and weaker.
After surgery, your physician may send you to physical therapy with instructions to guide healing and gradually return to activity.
Can This Injury or Condition Be Prevented?
Cubital tunnel syndrome is strongly linked to prolonged pressure at your elbow, repetitive elbow movement, and keeping your elbow bent. Awareness of how you use your arm throughout the day and changing your arm position if you notice changes can help prevent the onset of CuTs.
Once symptoms develop, the sooner you stop the symptoms, the better. If your hand has weakness from CuTs, then your recovery time may take longer, and there is a risk of long-term weakness in your hand. A check-in with a physical therapist or your physician if symptoms begin to recur could help you make adjustments at work or in your daily activities to help to prevent the condition or prevent it or keep it from getting worse.
What Kind of Physical Therapist Do I Need?
All physical therapists are prepared through education and experience to treat a variety of conditions, including cubital tunnel syndrome. You may want to consider the following:
- A physical therapist who is experienced in treating people with cubital tunnel syndrome. Some physical therapists focus on treating elbow, wrist, and hand (upper extremity) conditions.
- A physical therapist who is a board-certified clinical specialist or who completed a residency or fellowship in orthopedic physical therapy. These physical therapists have demonstrated advanced knowledge, experience, and skills that may apply to your condition.
- A physical therapist who is a board-certified clinical specialist or who completed a residency or fellowship in hand therapy (a certified hand therapist). This physical therapist has advanced knowledge, experience, and skills that may apply to your condition.
You can search for physical therapists near you who meet these criteria by using Find a PT, provided by the American Physical Therapy Association.
General tips when you're looking for a physical therapist (or any other health care provider):
- Ask family, friends, or other health care providers to recommend a physical therapist.
- Ask about the physical therapists' experience in helping people with cubital tunnel syndrome when you contact the clinic for an appointment.
- Be prepared to describe your symptoms in as much detail as possible. Make a note of what makes your symptoms better or worse.
The American Physical Therapy Association believes consumers should have easy access to clear, reliable information that helps them make informed health care decisions and feel prepared for visits with their providers.
The following resources offer the best scientific evidence on the physical therapy treatment of cubital tunnel syndrome. They cover recent research and standards of practice in the United States and globally. Whenever possible, they link to PubMed* abstracts (some of which offer free full-text access) or to other resources. You can read them to learn more or share them with your health care provider.
Chauhan M, Anand P, Das JM. Cubital Tunnel Syndrome. StatPearls [Internet]. StatPearls Publishing; 2025. Article Summary in PubMed.
American Academy of Orthopaedic Surgeons. Ulnar nerve entrapment at the elbow (cubital tunnel syndrome). Updated April 2024. Accessed September 16, 2025.
American Society for Surgery of the Hand. Cubital tunnel syndrome. Updated 2023. Accessed September 16, 2025.
Anderson D, Woods B, Abubakar T, et al. A comprehensive review of cubital tunnel syndrome. Orthop Rev (Pavia). 2022;14(3):38239. Article Summary in PubMed.
Nakashian MN, Ireland D, Kane PM. Cubital tunnel syndrome: current concepts. Curr Rev Musculoskelet Med. 2020;13(4):520-524. Article Summary in PubMed.
Andrews K, Rowland A, Pranjal A, et al. Cubital tunnel syndrome: anatomy, clinical presentation, and management. J Orthop. 2018;15(3):832-836. Article Summary in PubMed.
Assmus H, Antoniadis G, Bischoff C, et al. Cubital tunnel syndrome: a review and management guidelines. Cent Eur Neurosurg. 2011;72:90-98. Article Summary on PubMed.
*PubMed is a free public website run by the National Library of Medicine. It allows people to access summaries and references from health research articles published in scientific journals, including those indexed in the MEDLINE database.
Expert Review:
Sep 17, 2025
Revised:
Sep 17, 2025
Content Type: Guide
Cubital Tunnel Syndrome
PT, DPT, MS
Makenzie Mazin, PT, DScPT